WCRI’s 35th Annual Issues & Research Conference Part 1
February 28, 2019 in Phoenix, AZ
Live blogging by Yvonne Guibert
Dr. John Ruser, WCRI: Welcome and kick off to conference
For 8th year in a row, increased attendance. This year over 450 attendees!
This year’s theme: Breaking down barriers to improved IW’s outcomes.
WCRI donating $2 for every conference evaluation turned in during the conference.

WCRI Session 1: Policies Affecting the Workforce Now and in the Future

Professor Alan Krueger, Princeton University
Photo Credit: Princeton University
Opioid Crisis and the Workforce
Drugs are hitting the heart of the US workforce and are hitting males more significantly than female workers. In 2017 over 70k died of a drug overdose; over triple since 2002. (see slide 1) 70% of these due to opioids.
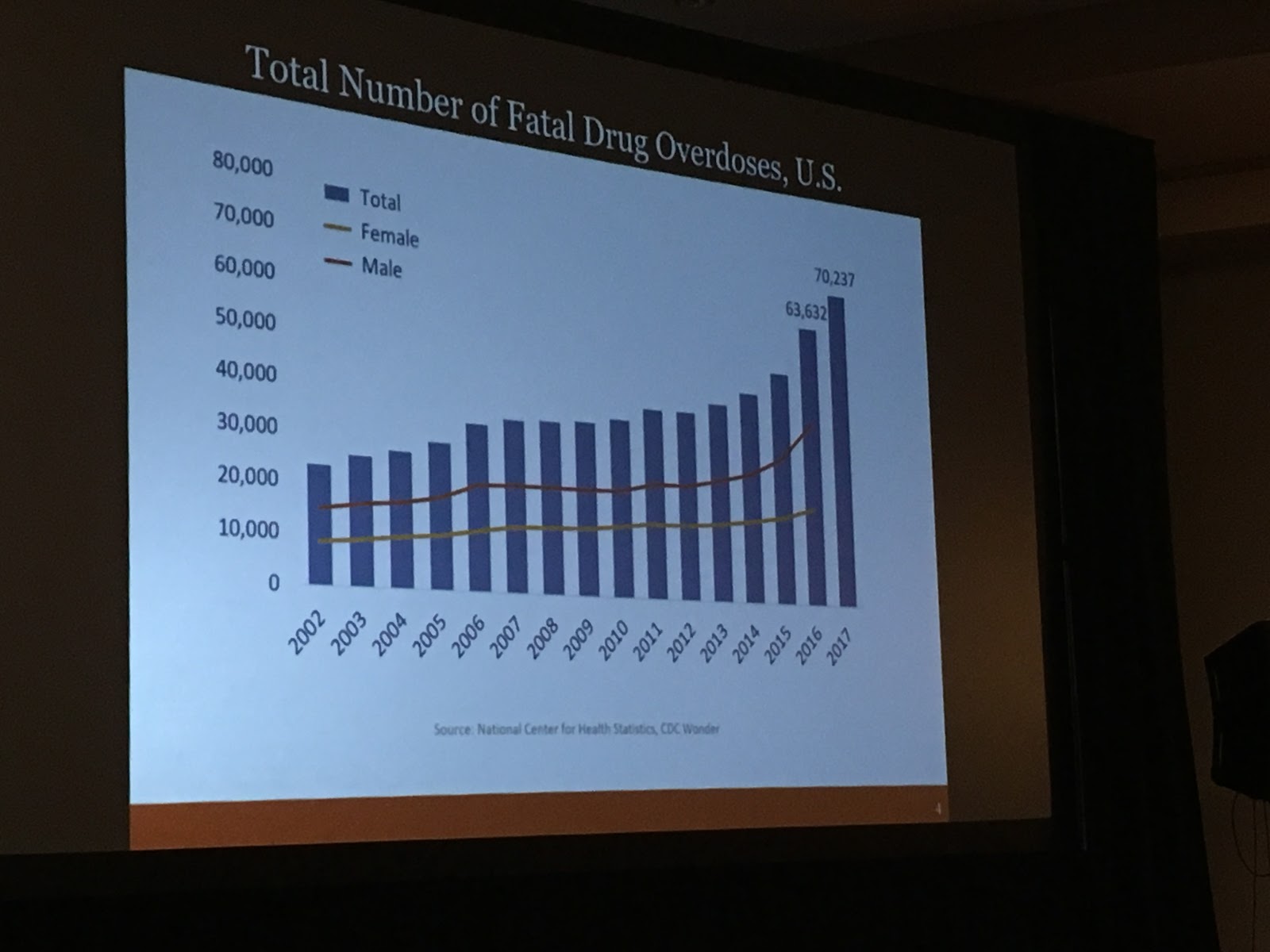
Slide 1 - WCRI 2019
White American mortality is a global outlier. What is driving this?
Deaths of despair are greater among less educated in the US.
Fentanyl is drug most often involved in overdose death 1999 - 2017 (see slide 2) by almost double. Next most common drug is heroin, followed by prescribed opioids.

Slide 2 - WCRI 2019
Causes of opioid crisis
- Recognition by medical community that pain is debilitating for many people
- Pharma companies encourage opioid scripts
- American doctors greatly overprescribe opioids compared to other countries
- Stody by Janet Currie / Molly Schnell: Doctors trained at the lowest-ranked med schools, write more opioid scripts than doctors trained at the highest ranked schools; results suggest better training for physicians, esp. general practitioners, could help curb the nation’s opioid epidemic -- the US would have had 56.5 percent fewer opioid scripts and 8.5% fewer overdose deaths if all general practitioners had prescribed opioids at the same rate as those from the top-ranked school (Harvard).
- Americans with diminished economic expectations are particularly vulnerable
- Addiction caused by prescription pain meds leads to demand for powerful illegal drugs e.g. heroin and fentanyl.
Labor force participation rate of prime working age men has trended down since WWII and is below 90%
Women participation has trended up -- peaked around 2000; then trended down over 2000’s; recently started trending up again, currently around 75%
Alan: for the US to continue economic growth, we need to be able to attract and retain workers
Many Non Labor Force (NLF) Prime Age Men Report Poor Health
More than ⅓ of NLF Men Report a Severe Disability
Nearly 20% report difficulty walking or climbing stairs19% of men report multiple disabilities
Pain Medication by Gender and Labor Force Status
Percent who took pain meds the previous day, ages 25-54 (see slide 3):
Employed:
20% men | 25%+ women
Unemployed:
19% men | 29% women
Not in Labor Force (not employed and not seeking employment)
35% men | 44% women
35% men | 44% women

Slide 3 - WCRI 2019
Longitudinal Princeton Pain Survey (PPS) (Fall of 2016 and Summer of 2017)
Surveyed 571 of NLF prime working age
47% of NLF prime-age men took pain meds on previous day
65% of those who took meds reported that they took prescription
Second Wave of PPS (conducted Summer 2017)
Add’l ?’s on how they pay for pain meds / scripts; source of pain; program participation
30% not on SSDI have applied for it; so around ½ of NLF prime age men are on or have applied for SSDI
There is no evidence that pain has declined despite opioid use
Underestimated Cost of the Opioid Crisis
Value of a Statistical Life -- about $10 million*
*involves many assumptions (e.g. extrapolation, rational choices, etc.)
Economic Costs
Estimated cost of opioid-involved overdose deaths in 2015
$500 billion annual cost 2015
Over 50% more fatalities in 2017, so cost could exceed $750 billion
Public Policy
- Declare public health emergency
- Limit # pills prescribed
- Alternate treatments for pain (e.g. phys therapy)
- More drug courts; treat addiction as a health problem
- More treatment slots for those addicted
- Better emergency room treatment for those overdosing
- Philippines: tough on drug dealers
- Portugal: controlled markets dispense methadone, etc.
- State and city lawsuits against pharmaceuticals
- Beware of next drug epidemic
Dr. John Ruser delved into some of the points Alan discussed.

Photo of Alan Krueger and John Ruser by Y. Guibert
John to Alan: what can we do to address this problem with opioids in USA?
Alan: I think we need a two-pronged strategy:
1- affect flow into addiction
2- treatment help for those addicted
John: tell us about your work with US government
Alan: The current political environment is the flip side of what we saw in 2011-2014. People forget that the house was controlled by Republicans and senate by Democrats. So when there’s gridlock...regardless of who controls what, it is hard for the government to do more than the bare minimum when the government is divided:
Passing a balanced budget
Raise the debt ceiling
Operating in a deficit
Congress has another constraint
On trade deals with current administration...Trump admin has negotiated with China. There are legitimate issues that US needs to negotiate with China. Worries about what will happen with NAFTA; difficult for congress to address. Difficult politics with little room / ability to make progress.
John: When will economic growth period end?
Alan: if we get past this summer then it will be longest ever growth period (surpassing the 1990’s).
What causes a recovery to end? Raising interest rates too high. Federal reserve very aware of this in history. Less likely that fed. Reserve will take action that ends the recovery. Other factors: foreign wars, financial crises. Concern of late is that when the next crisis does hit, the tools that the US government has are minimal. Fed. reserve can only lower interest rates so much. Fiscal policy / stimulus. Deficits close to a $ trillion per year.
Odds of a recession. In any given year a 20-25% chance that a recession could emerge. Trend growth over last 9.5 years has been slightly below 2% per year. About what you’d expect from sluggish productivity growth. Mainly driven by short term stimulus -- corporate tax cuts, etc. That will fade out. Last qtr of 2018 GDP 2.6% slightly above projections. Projections for 1st qtr this year closer to 1-1.5%.
“Recoveries don’t die of old age, they get murdered.” Prof. Alan Krueger quoting Bernanke
John: shift focus to labor market. Experts say automation should bring as many jobs as it eliminates. What are your thoughts about this?
Alan: no one really knows. Economists have a terrible track record. Tremendous amount of movement when you look at how many jobs eliminated vs. how many created. There are a lot of cross currents. Important to understand what skills are needed; what industries; how do we prepare the workforce to be ready for future jobs.
Productivity has slowed...partly due to aging workforce. Not optimistic about the nature of the job growth.
Alan: focus on intermediaries in the workforce
WCRI Session 2: Latest Research & Efforts to Address the Opioid Epidemic
This session addressed research and efforts related to the opioid epidemic.
Moderator: Mr. Tim Hassett-Salley, WCRI
Dr. Vennela Thumula, WCRI
Dr. Letitia Davis, MA Dept of Public Health
Ms. Jacqueline Kurth, Industrial Commission of AZ
Mr. Jason Porter, Industrial Commission of AZ

Photo of WCRI Session 2 Panel by Y. Guibert
Dr. Vennela Thumula, presented an overview of WCRI Research, which identifies characteristics (age, locations,industry, injury type, etc.) of injured workers and their employers that are associated with differences in opioid dispensing rates
+Older workers received slightly more opioid prescriptions than younger workers. 42% of workers age 23-38 received an opioid prescription vs. 49% of workers over age 55.
+Construction and mining workers had a higher % of opioid prescriptions as compared to 11 other industries.
Higher Rate of Opioid Rx seen in workers who were:
- Older
- Male
- Residing in rural areas
- Residing in counties with higher MME prescribing per capita
- Employed in mining, construction
- Employed in smaller firms
- Sustained fractures, carpal tunnel, neurological spine pain injuries
Dr. Letitia Davis -- Massachusetts Study
Dr. Davis discussed results from a recent study published.
She said there is an epidemic in MA...the rate of opioid overdoses / deaths almost double compared to other states
Goal of study: describe opioid-related overdose deaths among MA residents by industry and occupation (by gender, race / ethnicity)
- Data source: MA death certificates 2011-2015
- Excluded deaths: retired, unemployed, disabled, housewife, no occupational info
- Rates: overdose deaths per 100K workers
The study found that there were 4,301 opioid deaths of employed persons. In construction and fishing industries, overdose and death rates were six times the rate of other industries. Occupations with the highest injury rates also showed the highest overdose death rates.
What is not known from the study / data reviewed is whether or not people who died from opioid overdoses were prescribed those drugs due to a workplace injury.
Conclusion: more research is needed to understand the correlation of workplace injuries and other occupational factors to opioid use and overdose deaths.
Jason Porter -- Arizona Efforts
June of 2017, governor declared of emergency re: opioid overdoses based on the fact that AZ experienced an opioid overdose death rate higher than ever seen before. Governor required increased research and legislation to address the issue.
Some of the new legislation passed included significant restrictions on physician dispensing, requiring pharmacies to check the PDMP before dispensing and limited initial fill to 5 days. Launched a hotline for healthcare providers with information about opioid prescribing. Doctors in AZ are required to submit a tapering plan. Also increased licensing requirements of pain management facilities to be commensurate with other healthcare facilities.
Early results show over 35% decrease in opioid prescriptions significantly less doctor shopping, an increase in overdoses referred to behavioral health providers and nearly 80% reduction in the number of patients receiving prescriptions over 90 pills.
Jacqueline Kurth -- AZ Legislative Changes to Address Opioid Epidemic
April 2012, AZ lawmakers passed House Bill 2368 which required Industrial Commission to “develop and implement a process for the use of evidence-based treatment (EBM) guidelines, where appropriate, to treat injured workers.”
Director created an EBM Advisory Committee; comprised of a diverse group of stakeholders
Advisory Committee Goals
3 objectives:
- Extensive / exhaustive research on treatment guidelines
- Conduct stakeholder survey about treatment guidelines
- Hear from subject matter experts
Following recommendations:
- Limit guidelines to management of chronic pain and use of opioids for all stages of pain mgmt
- Adopt existing guidelines (vs. drafting an AZ specific guideline)
- Asked group of medical specialists to evaluate the various guidelines available
Committee ultimately adopted ODG guidelines
Treatment guidelines were expanded to all body parts and conditions in October, 2018.
Dec 2017 - commission determined that modifying the applicability of ODG to cover all body parts and conditions would improve medical treatment for IWs and would make treatment and claims processing more efficient and cost effective.
Change in Oxycodone Pill Equivalents by Claim Maturity by Service Year 2016-2017 (NCCI Data)
After 1 year, have seen significant changes in OPE from SY 2016-2017
Our goal in AZ is to reduce opioid deaths and to improve the quality of life for AZ workers.
Question from Gary Anderberg, Gallagher Bassett: “Why have ALL states not adopted treatment guidelines? Where is the resistance coming from?”
Mark Walls said via Twitter: “Panel won’t say it, but I will. When things don’t make sense, follow the money. Who benefits from the inappropriate prescribing of opioids?”
WCRI Session 3:
From Washington State to Washington DC -- A Model for Coordinated RTW Services
Moderator: Dr. John Ruser, WCRI
Speakers:
Prof. Tom Wickizer, University of Washington School of Public Health
Ms. Jennifer Sheehy, US Dept of Labor’s Office of Disability Employment Policy (ODEP)

Photo of WCRI Session 3 Panel by Y. Guibert
Key Lessons:
Efforts to improve Stay-at-work / Return-to-Work outcomes
SAW/RTW Policy Collaborative
- Launched in 2013
- Community of Practice
- Disability management experts
- Employers and industry associates
- Worker Associates
- Public Sector Entities
- Researchers
- Policy Work Groups
- Led by SMEs
- Informed by CoP
- Landscape Analysis
- National Online Dialogues
- Policy Recommendations
- Resources to Support Adoption and Implementation
Timing is everything
- Intervene at appropriate time
- Ideally, while IW is still attached to the employer
Outreach and coordination are critically important:
RETAIN (Retaining Employment and Talent After Injury / Illness Network)
- RETAIN will serve workers to prevent work disabilities by funding these strategies
- Training in occupational health best practices (including non-opioid pain management)
- Active involvement of a RTW coordinator
- Enhanced communication among workers, employers and health care providers
- Accommodations and job modifications
- Retraining and rehabilitation services
- Projects will provide services through an integrated network of partners that includes state and/or local workforce development entities, health care systems and other partners
Project Timelines
RETAIN projects will span a total of 5 years and will be funded in two phases:
Phase 1 -- Planning and Pilot
- 18 months and include planning and start-up activities including launch of small pilot demonstration within nine months of award
- Nearly $19 million was awarded to 8 state workforce agencies for Phase 1
Phase 2 -- Implementation
- 42 months and includes full scale implementation
- A subset of Phase 1 awardees will be competitively selected to receive up to $19.75 million each
RETAIN Phase 1 Recipients: CA, CT, KS, KY, MN, OH, VT, WA (see slide 4)

Slide 4 -- WCRI 2019

Comments
Post a Comment