WCRI 2019 Annual Conference, Day 2 | Phoenix, AZ
WCRI 2019 Annual Conference, Day 2 | Phoenix, AZ
On the second day of the 2019 WCRI Annual Conference, the first session
On the second day of the 2019 WCRI Annual Conference, the first session
discussed findings and trends of several WCRI studies. State of the States:
Selective Findings session included the following speakers:
Moderator: Ramona Tanabe, WCRI: Facility Metrics
Speakers:
Selective Findings session included the following speakers:
Moderator: Ramona Tanabe, WCRI: Facility Metrics
Speakers:
Carol Telles, WCRI
Evelina Radeva, WCRI
Rebecca Yang, WCRI

WCRI Day 2 Session 1 Panel of Speakers | Photo by Y. Guibert
Facility payments are seen in 26-44% of total claims and represent 9-25% of
Facility payments are seen in 26-44% of total claims and represent 9-25% of
medical payments across 18 states studies. The median was 17%. There was
a wide variation in % of medical payments for facility services by billed place
of service. (see Facility slide 1)
a wide variation in % of medical payments for facility services by billed place
of service. (see Facility slide 1)

Facility Slide 1 | Photo by Y. Guibert
Ambulatory surgery center (ASC) fees ranged from 4% in MA to 25%
in NJ; hospital outpatient fees ranged from 10% in CA to 31% in WI;
the average facility payment per claim in the highest states is 4-5x that
of lowest states. This was attributed to different reimbursement rules
for facilities across the states studied. (see Facility slide 2)
in NJ; hospital outpatient fees ranged from 10% in CA to 31% in WI;
the average facility payment per claim in the highest states is 4-5x that
of lowest states. This was attributed to different reimbursement rules
for facilities across the states studied. (see Facility slide 2)

Facility Slide 2 | Photo by Y. Guibert
There was a decrease in inpatient care and a shift from hospital outpatient
to ASC facilities during the period 2011 - 2016. It was noted that NC legislation
changed their reimbursement fee structure during the study period. The
new fee structure went into effect in 2015.
to ASC facilities during the period 2011 - 2016. It was noted that NC legislation
changed their reimbursement fee structure during the study period. The
new fee structure went into effect in 2015.
Facility payments make up a sizable share of medical payments in many states
30-35% of claims with major surgery in most states at 12 months; 35-40% at 36
months.
months.
The study found there was a slight decrease in major surgeries: includes invasive
surgery ranging from 2-5% in many states 2011-2016.
surgery ranging from 2-5% in many states 2011-2016.
Possible reasons for decrease in surgery rates:
- Alternatives to surgery
- State-specific initiatives and active payor management
- Change in the injury mix
The percent of low back disc cases with surgery decreased in most of the
study states.
study states.
Evelina Radeva, WCRI: Benefit Delivery Expenses
Study on Benefit Delivery Expenses (BDE)
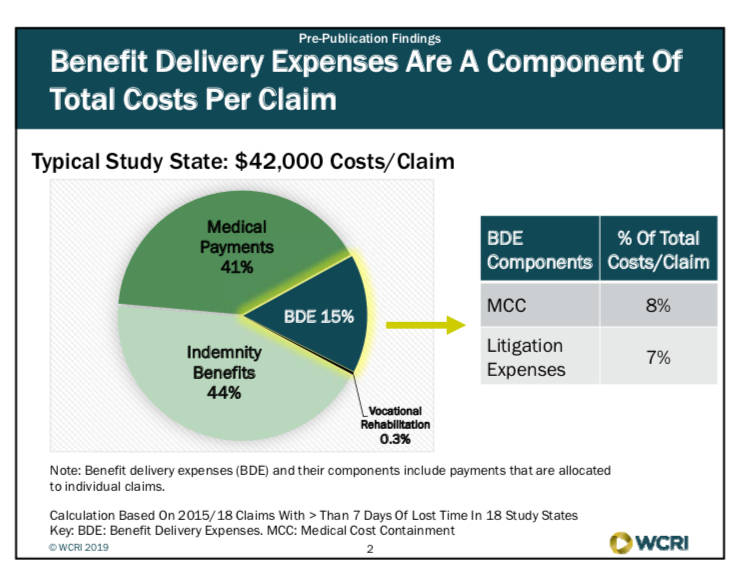
Average claim for minimum 7 days lost time = $42,000. In addition to
medical and indemnity expenses, BDE cost make up a significant portion
of the claims in workers’ comp. In a typical state, indemnity costs
made up 44% of total costs, medical was 41% and BDE was 15%.
(see BDE Slide 1) About half the BDE costs were made up of litigation,
the other half were made up of medical management fees, e.g. bill review,
UR and nurse case management.
medical and indemnity expenses, BDE cost make up a significant portion
of the claims in workers’ comp. In a typical state, indemnity costs
made up 44% of total costs, medical was 41% and BDE was 15%.
(see BDE Slide 1) About half the BDE costs were made up of litigation,
the other half were made up of medical management fees, e.g. bill review,
UR and nurse case management.
BDE Slide 1
BDE expenses are made up of mostly two types of services:
Medical cost containment
- Bill review
- Utilization review
- Case management
- Provider networks
- Defense attorney payments
- Medical-legal expenses (IMEs, medical testimony, depositions)
- Other (copying, transcription fees, interpreters)
Across the states included in the study BDE accounted for 11% (WI) - 23% (CA)
of total costs per claim in 2015 / 2018. In dollars, fees ranged from $4208 on
the low end (WI) and the high end, nearly $12,000 per claim (LA).
of total costs per claim in 2015 / 2018. In dollars, fees ranged from $4208 on
the low end (WI) and the high end, nearly $12,000 per claim (LA).
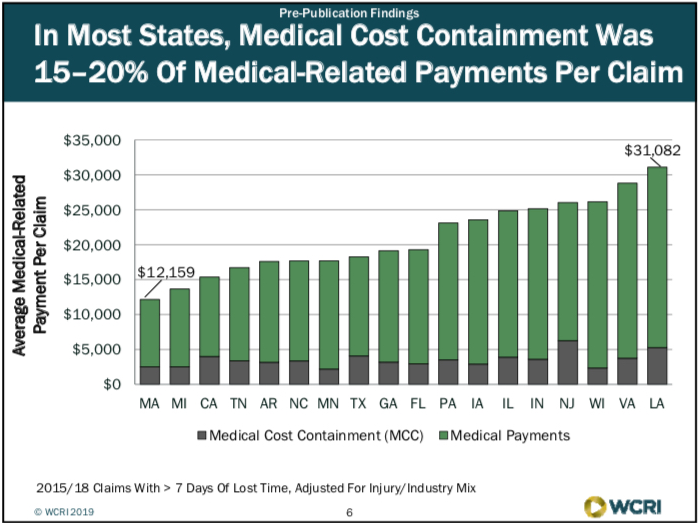
In most states, medical cost containment was 15-20% of medical-related
payments per claim
payments per claim
Ranging from $12k in MA to $31k in LA (see BDE Slide 2).
BDE Slide 2
It was noted that the variance in fees was likely due to the different
medical cost containment strategies employed among the study states:
medical cost containment strategies employed among the study states:
- Medical fee schedules
- Pharma fee schedule
- Treatment limits
- Utilization review
- Treatment guidelines
- Managed care
- Choice initial provider
Defense attorney payments were the largest share of litigation expenses in most states with fees ranging from $2.8k in TX to $9.5k in LA (See BDE slide 3). Texas system includes ombudsmen to assist injured workers amongst other resources which has resulted in greatly reduced litigation fees.

BDE Slide 3
System features driving differences in litigation expenses per claim among states
- Are participants able to easily navigate the system?
- Informal vs. formal dispute resolution process
- Design of the process to determine whether PPD benefits will be awarded, and the level of benefits
- State agency monitoring of dispute resolution and timelines of first temporary total disability payment
BDE per claim grew about 4-6% since 2005 in most study states; NJ and
LA had highest increases among the study states; MN had the least increase.
LA had highest increases among the study states; MN had the least increase.
Median Study State: small growth in % of claims with litigation services;
payments grew 4-6% / year since 2005
payments grew 4-6% / year since 2005
Key Findings
- BDE were 11-23% of total costs per claim among study states in 2015 (evaluated 2018)
- Average BDE per claim affected by medical cost containment strategies, system features and dispute resolution process
- BDE per claim grew about 4-6% per year in most study states 2005-2015 (at 36 months)
Rebecca Yang, WCRI: Frequency and Cost of Lump-Sum Settlements
Rebecca presented findings on WCRI’s study of frequency and costs of
lump-sum settlements. Of the states reviewed there were generally two
types of indemnity benefit systems: Wage-Loss vs. PPD and 2 states that
represented a hybrid of both. (See Lump Sum Slide 1)
lump-sum settlements. Of the states reviewed there were generally two
types of indemnity benefit systems: Wage-Loss vs. PPD and 2 states that
represented a hybrid of both. (See Lump Sum Slide 1)
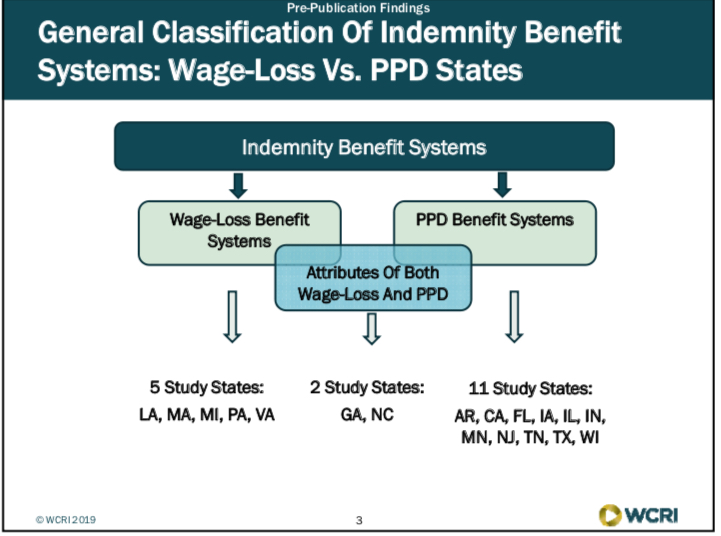
Lump Sum Slide 1
Wage Loss Benefit Systems: 5 Study states: LA, MA, MI, PA, VA
PPD Benefit Systems: 11 study states: AR, CA, FL, IA, IL, IN, MN, NJ,TN, TX, WI
Attributes of Both wage loss and PPD: 2 study states: GA, NC
State variation in frequency and amount of lump-sum settlements
reflects the benefit structure and other factors, e.g. states with
wage-loss benefit systems had higher settlement amounts.
reflects the benefit structure and other factors, e.g. states with
wage-loss benefit systems had higher settlement amounts.
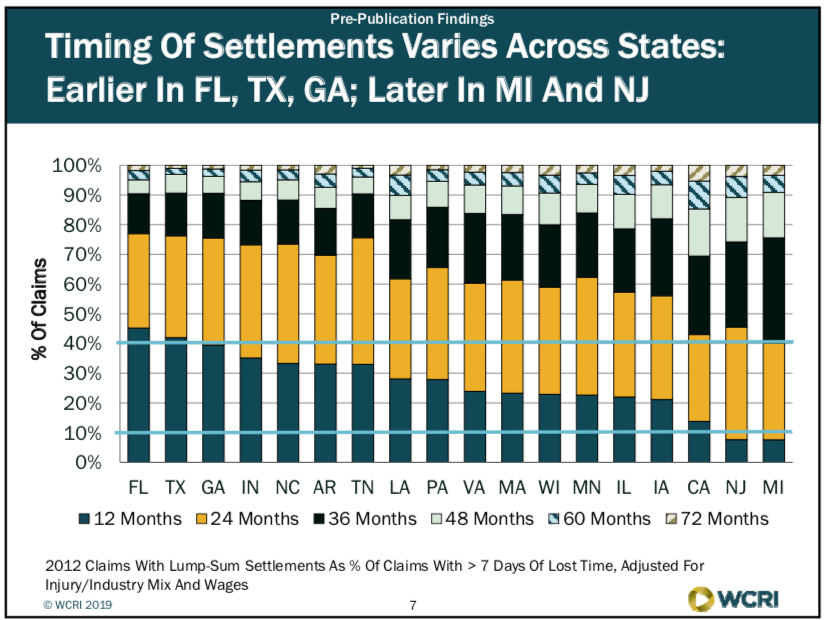
Timing of settlements varies across states: were earlier in FL, TX, GA;
later in MI and NJ (see Lump Sum Slide 2)
later in MI and NJ (see Lump Sum Slide 2)
Lump Sum Slide 2
Factors that may influence trends in lump-sum settlement frequency and
costs in WC claims:
costs in WC claims:
- Policy changes addressing income benefit payments
- Change in speed of dispute resolution, settlement approval or attorney involvement
- Change in factors that influence workers, payors and attorneys to seek settlements
The percent of claims with lump-sum settlements increased in most
study states since 2008. Settlement amounts per claim remained stable in most states.
study states since 2008. Settlement amounts per claim remained stable in most states.
CA: longer term increase in lump sum frequency; earlier settlements post SB 863.
FL: faster recent growth in settlement amounts may be related to early
effect of court decisions.
effect of court decisions.
WCRI Day 2 | Session 2: Challenges & Opportunities of Telemedicine
Moderator: Dr. David Deitz, David Deitz & Associates
Speakers: Ms. Amy Lee, Texas Dept of Ins
Mr. Kurt Leisure, The Cheesecake Factory
Mr. Dan Allen, Construction Industry Service Corp (CISCO)
Dr. Stephen Dawkins, Caduceus USA
I appreciated the creative and engaging method WCRI used to draw
the attendees back into the session room from the break. They played
a video clip from the movie Casino Royale...the James Bond poisoning scene...
he used a remote monitor to restart his heart.
the attendees back into the session room from the break. They played
a video clip from the movie Casino Royale...the James Bond poisoning scene...
he used a remote monitor to restart his heart.
Telemedicine: What we don’t know:
- No quantitative data on use in wc
- Quality trade-offs: most QOC data are “non inferiority”
- Appropriate regulations and reimbursement models?
- Privacy, liability, employee choice, etc.
The Cheesecake Factory launched telemedicine approximately one year ago.
Telemedicine -- the process:
- Injury occurs
- If 911 - proceed to Urgent Care / ER
- If non-urgent:
- Nurse triage
- If unsuccessful and non-emergent, escalate to Telemedicine via mobile device
- If telemedicine fails, proceed to UC, ER
Potential Benefits for EE:
- Immediate medical care -- no waiting room
- Flexibility of treatment - another option
- 24 hours a day / 7 days a week accessible
- More focused attention from doctor
- No MRSA exposure
- Bilingual doctors available
- Rx to the pharmacy of ee’s choice
- RTW with minimal disruption -- may never have to leave the injury location
- Notes from nurse triage to transfer to tele Dr
- Mobile device obtains visual for Dr
Potential Benefits for Employer:
- No transportation issues
- Immediate care for valued ee
- Costs are set per call, less $ than UC/ER
- Injury notes transferred to intake system
- Measurable hard $ results
- No repricing fees
- Keeps ee away from med/legal mills
- Financial savings could be significant
- Medical care is consistent with group ins benefits
- No need to cover shift or pay thru end of shift
Potential Risks:
- Program not successful -- too many claims referred to UC/ER from telemed
- Wi-Fi or camera expense / connectivity (not an issue for Cheesecake)
- Privacy concerns -- need a private location (office / restroom)
- Adoption by injured staff
YTD Actual Results for Cheesecake (Feb 2018 implementation):
- 3,336 calls into nurse triage
- 1,078 successful triaged by nurse - 32%
- 470 (21%) of remaining 2258 injuries offered telemedicine by nurse triage
- 326 (69%) accepted telemedicine
- 188 (57%) successfully treated through telemedicine and needed no further treatment
- $153K in hard dollar savings in 2018
Opportunities / Lessons Learned / learning:
- Triage needs add’l algorithms to identify telemedicine candidates
- Will take time for staff to trust program
- Internal marketing
- Work with group ins telemed program
- Cultural trust issues
- Ipad concept was “clunky” cont’d automation is critical
- Approval by IWs is high
- More engagement by Dr
- Convenience factor is HUGE
Amy Lee - Texas Dept of Insurance
From the regulators perspective; issues that we have had to learn / grapple with...
Senate Bill (SB) 1107:
- Passed in 2017 (not a wc bill)
- Changed the way TX Med board regulated telemedicine services
- Required joint rulemaking between various practitioner licensing boards
- Included requirements for fully insured health plan
which include existing WC statutory requirements, billing and reimbursement
structure, evidence-based treatment guidelines and pharma formulary
(ODG in Texas), UR requirements, health care networks and dispute resolution.
structure, evidence-based treatment guidelines and pharma formulary
(ODG in Texas), UR requirements, health care networks and dispute resolution.
She then discussed Texas DWC rulemaking goals which is to promote statutory
system goals including:
system goals including:
- Provide timely, appropriate and high quality medical care to IWs to facilitate RTW
- Timely and cost-effective income and medical benefits
- Taking advantage of technology to provide highest levels of service
- Expand access to telemedicine using current medical billing and reimbursement structure
- Defer to state licensing boards on scope of practice issues
- Preserve IWs statutory choice of treating physician
- Provide clear guidance to healthcare providers and insurance carriers to
- Minimize fee disputes
- Enable data collection and outcomes tracking
- Address medical care -- not medical - legal examinations
Telemedicine Utilization in TX:
- Workers’ comp study planned for 2019
- Data since Sept 2018 still preliminary:
- Less than 100 claims
- 31 insurance carriers
- Fewer than 200 medical bills
- Mostly office visits / consultations
- Focus on non-rural areas of the state
or after September 1, 2018. For more information on this new Texas rule visit the TDI website here.
In closing, Amy discussed future policy considerations:
- Monitor changes to Medicare list of services that can be performed via telemedicine
- Evaluate impact of telemedicine on:
- Medical costs and utilization
- Access to care, especially underserved areas of Texas
- RTW outcomes and IW satisfaction
- Ensure medical data are collected and reported correctly to enabling tracking of costs and outcomes.
I had to scoot out early from this session to catch my flight as Amy was
wrapping up her discussion. So the remaining information here is culled
from the Twittersphere….
WCRI @WCRI: “Dan Allen from @CiscoBuildUnion says construction
WCRI @WCRI: “Dan Allen from @CiscoBuildUnion says construction
workers don’t have days off...so they may embrace telemedicine if they
can get the care they need fast.Younger workers may be open to it, but
older workers will probably reject it and opt for a traditional visit.”
can get the care they need fast.Younger workers may be open to it, but
older workers will probably reject it and opt for a traditional visit.”
Tom Kerr @Tomker11: “Dr. David Deitz said that 1/100th of recent patient
visits were done through telemedicine, where as much as 30% could be done
through telemedicine. So there is tremendous opportunity for growth.”
visits were done through telemedicine, where as much as 30% could be done
through telemedicine. So there is tremendous opportunity for growth.”
Insurance Research @III_Research: “It’s crystal clear [...] that telemedicine
is a tsunami that will change the practice of medical care.” Dr. Stephen Dawkins
gives a provider’s perspective on telemedicine.
is a tsunami that will change the practice of medical care.” Dr. Stephen Dawkins
gives a provider’s perspective on telemedicine.
Mark Walls @wcmarkwalls: “Takeaways from #WCRI19 telemedicine panel:
- Clear advantages with access to care, especially underserved areas.
- Know your goals. Not necessarily cheaper. But faster and more convenient.
- Regulatory challenges around scope of care and reimbursement.
- Employee adoption key.”
A day and a half of WCRI sessions presented by really smart people and filled
with fascinating data, research and observations. This is becoming one of my
favorite events of the year. I guess that means I’m becoming a WC nerd. Great
to see everyone! See you next year.
with fascinating data, research and observations. This is becoming one of my
favorite events of the year. I guess that means I’m becoming a WC nerd. Great
to see everyone! See you next year.

Comments
Post a Comment